Archival collection
Use this image
Can I reuse this image without permission? Yes
Object images on the Ingenium Collection’s portal have the following Creative Commons license:
Copyright Ingenium / CC BY-NC-ND (Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
ATTRIBUTE THIS IMAGE
Ingenium,
1981.0489.002
Permalink:
Ingenium is releasing this image under the Creative Commons licensing framework, and encourages downloading and reuse for non-commercial purposes. Please acknowledge Ingenium and cite the artifact number.
DOWNLOAD IMAGEPURCHASE THIS IMAGE
This image is free for non-commercial use.
For commercial use, please consult our Reproduction Fees and contact us to purchase the image.
- OBJECT TYPE
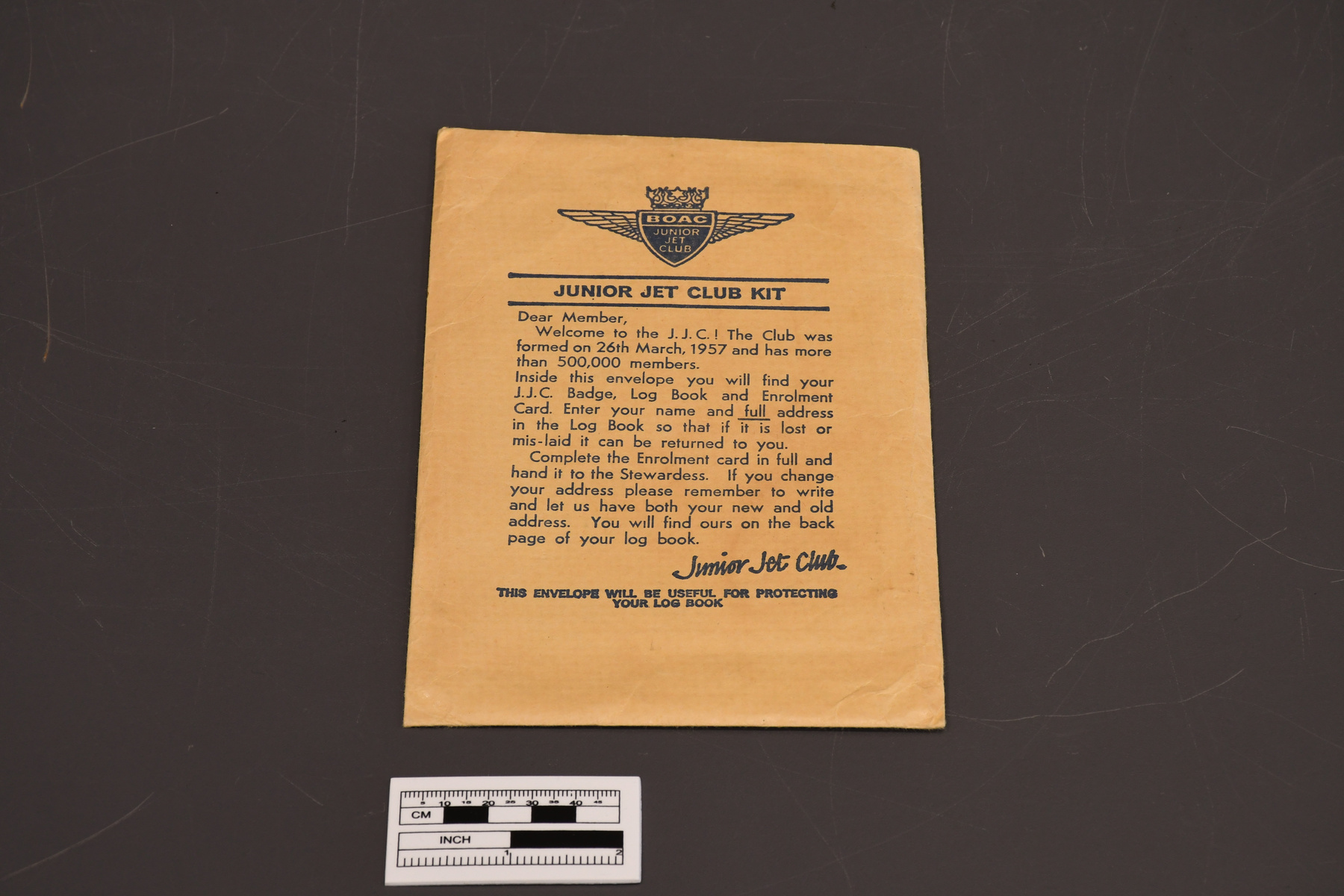
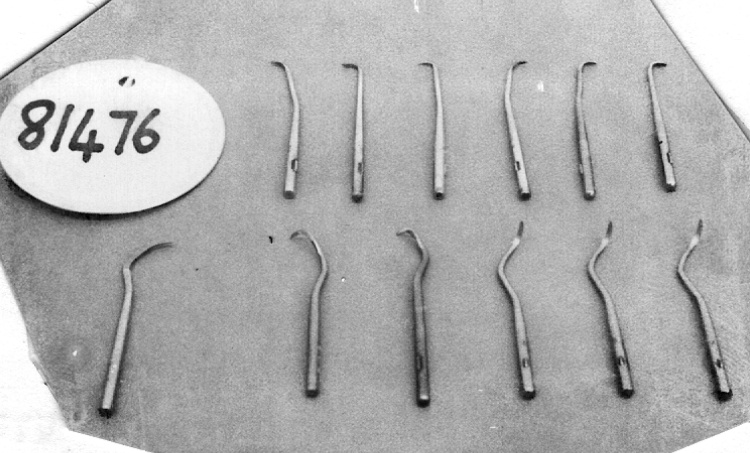
- DENTAL FORMS
- DATE
- 1920–1948
- ARTIFACT NUMBER
- 1981.0489.002
- MANUFACTURER
- Unknown
- MODEL
- Unknown
- LOCATION
- United States of America
More Information
General Information
- Serial #
- N/A
- Part Number
- 2
- Total Parts
- 2
- AKA
- form
- Patents
- N/A
- General Description
- PAPER.
Dimensions
Note: These reflect the general size for storage and are not necessarily representative of the object's true dimensions.
- Length
- 23.0 cm
- Width
- 16.0 cm
- Height
- N/A
- Thickness
- N/A
- Weight
- N/A
- Diameter
- N/A
- Volume
- N/A
Lexicon
- Group
- Medical Technology
- Category
- Archives
- Sub-Category
- N/A
Manufacturer
- AKA
- Unknown
- Country
- United States of America
- State/Province
- Unknown
- City
- Unknown
Context
- Country
- Unknown
- State/Province
- Unknown
- Period
- Unknown
- Canada
-
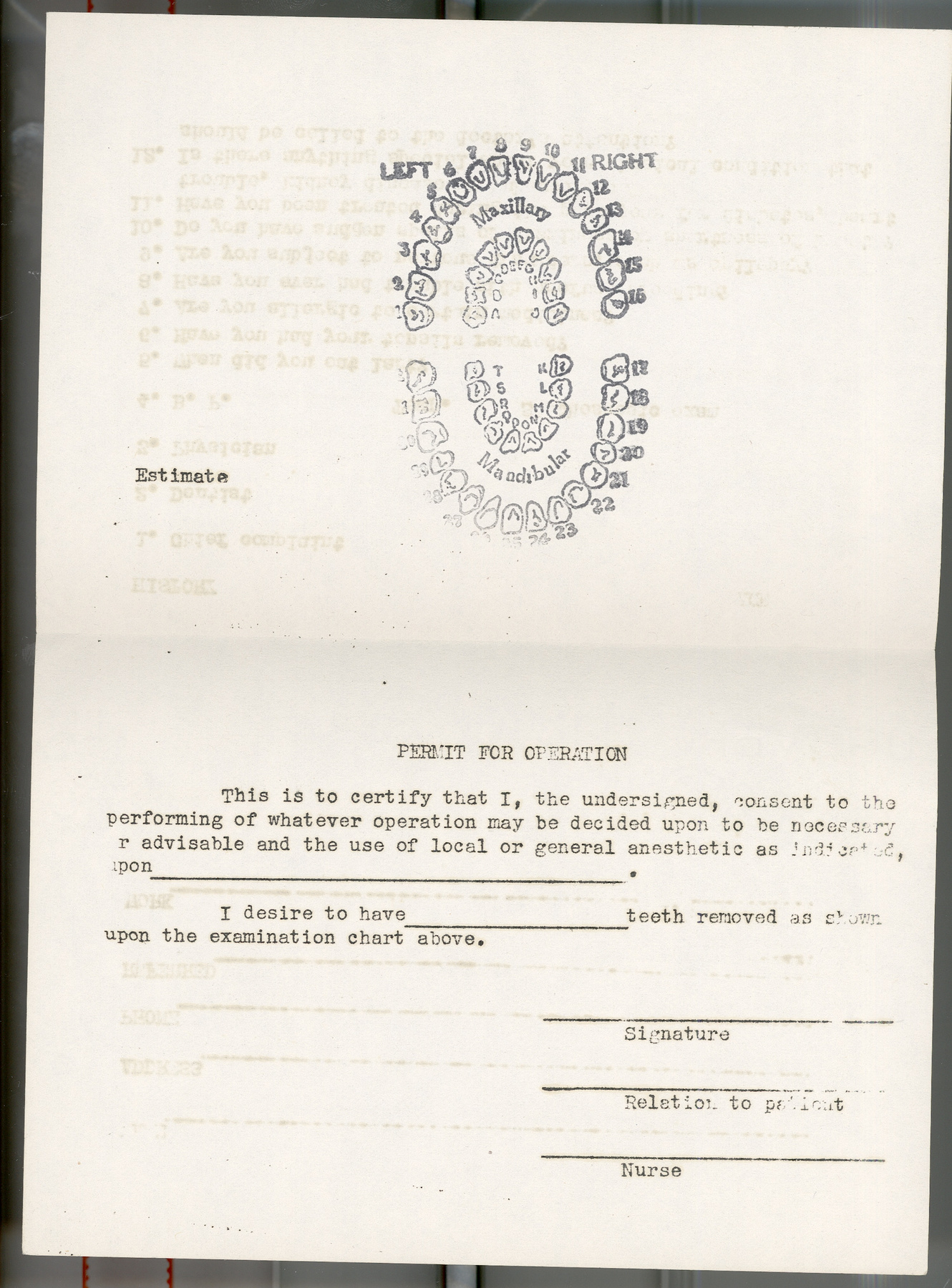
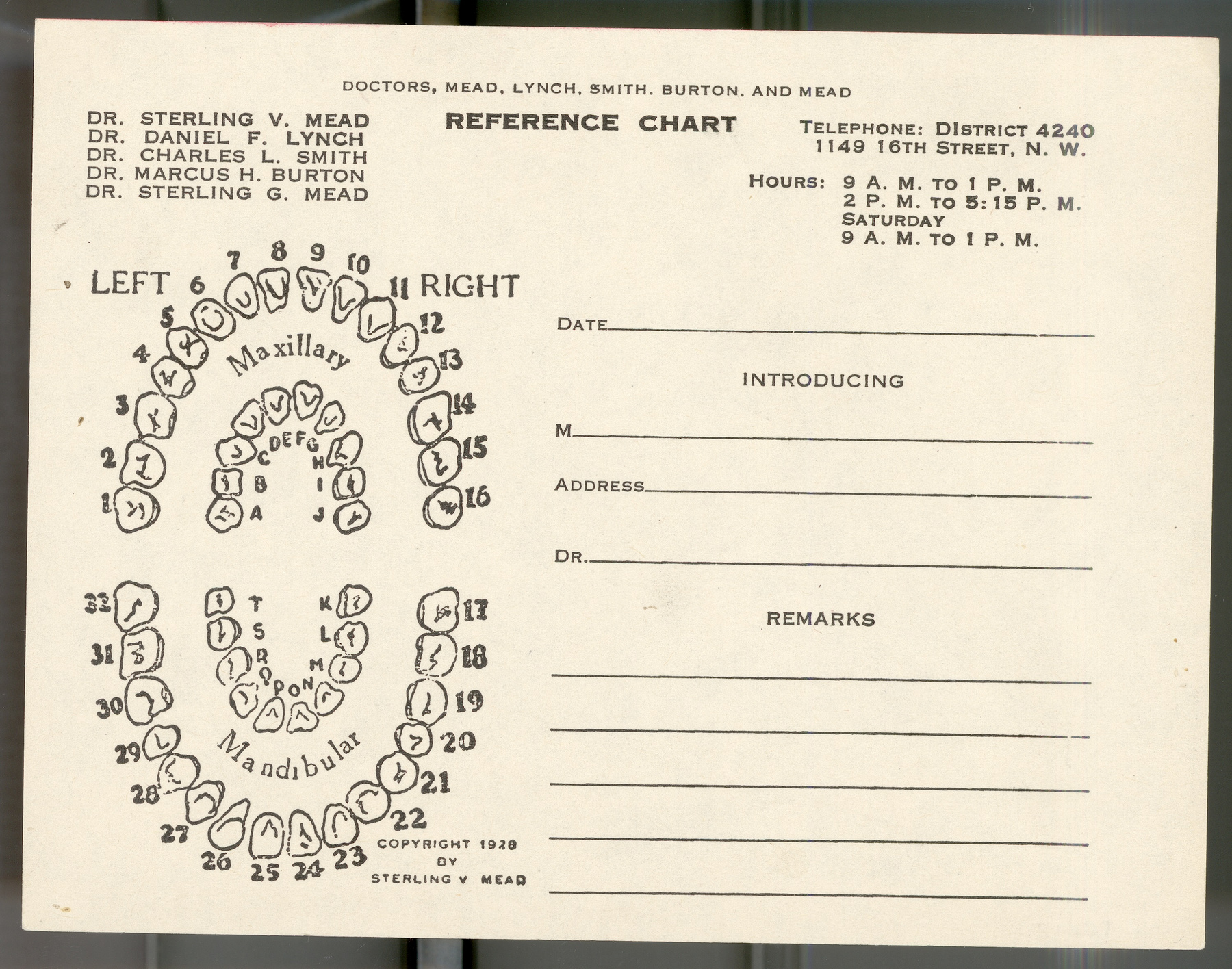
Samples of forms used by Drs. Mead, Lynch, Smith, Burton & Mead of Washington, DC and sent to donor in November, 1948. - Function
-
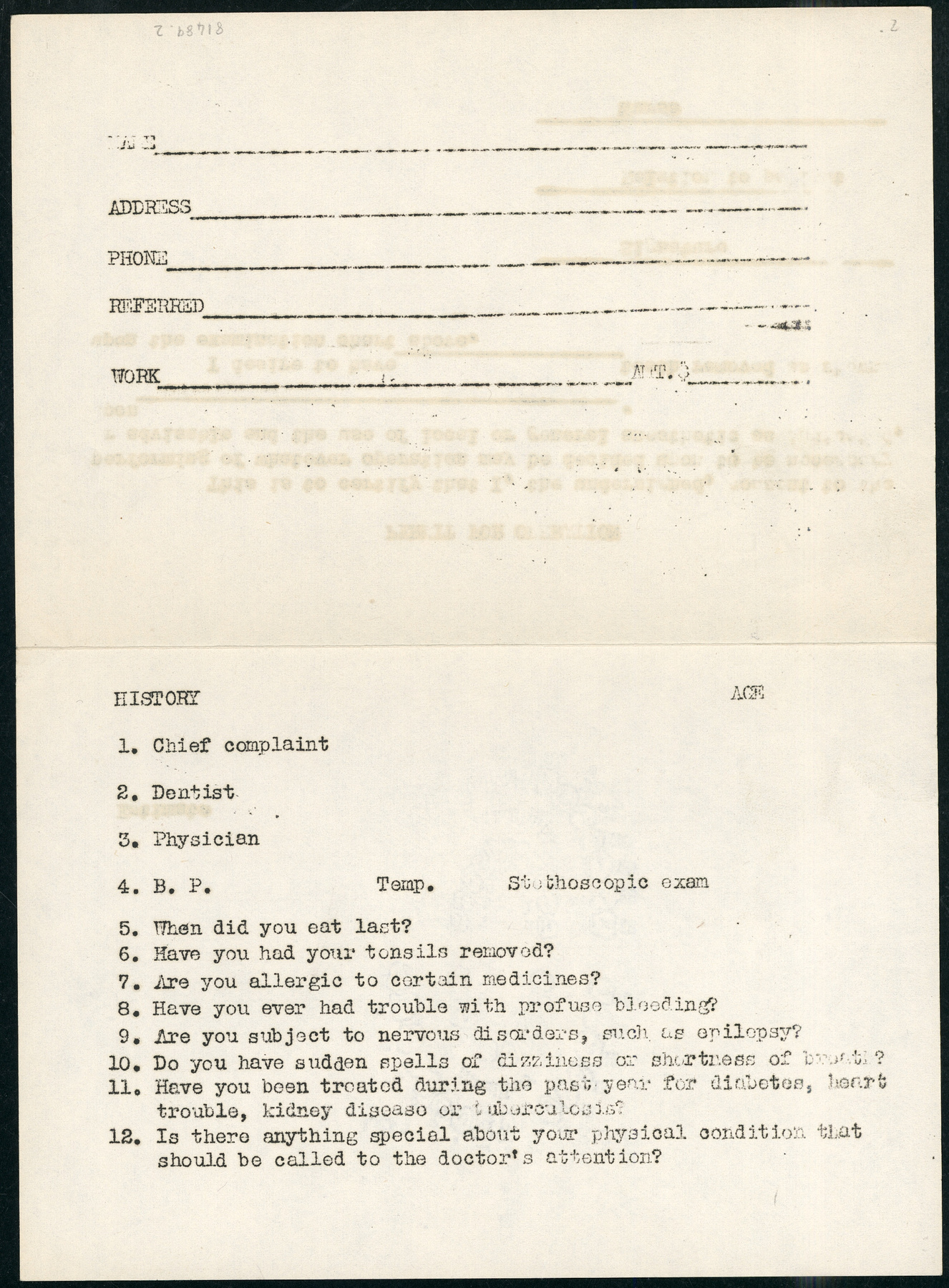
To record basic personal and medical information, and provide written proof-of-consent prior to treatment. - Technical
-
Unknown - Area Notes
-
Unknown
Details
- Markings
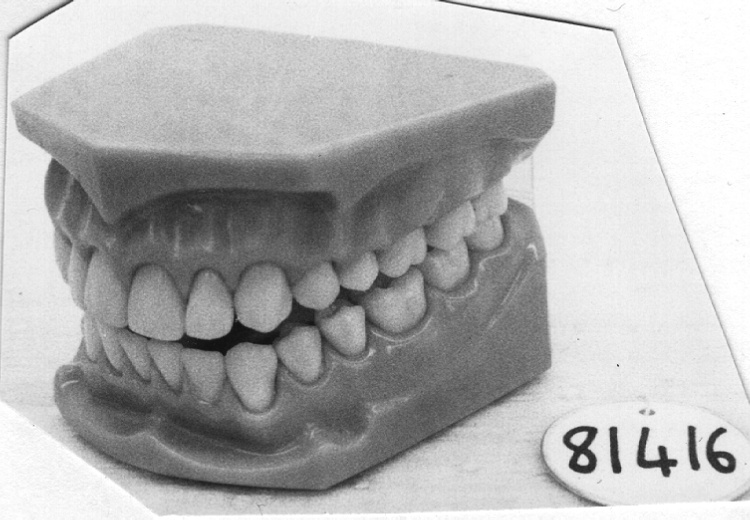
- Form features annotated illustration of standard arrangement of human teeth, and includes text " PERMIT FOR OPERATION/ This is to certify that I, the undersigned, consent to the/ performing of whatever operation may be decided upon to be necessary/ [o]r advisable and the use of local or general anesthetic as indicated,/ upon_________./ I desire to have____________ teeth removed at shown/ upon the examination chart above./ ________/ Signature/ _________/ Relation to patient/ _______/ Nurse". "NAME____________/ ADDRESS________/ PHONE___________/ REFERRED__________/ WORK____________AMT.$___________/ HISTORY AGE/ 1. Chief complaint/ 2. Dentist/ 3. Physician/ 4. B.P. Temp. Stethoscopic exam/ 5. When did you eat last?/ ^. Have you had your tonsils removed?/ 7. Are you allergic to certain medicines?/ 8. Have you ever had trouble with profuse bleeding?/ 9. Are you subject to nervous disorders, such as epilepsy?/ 10. Do you have sudden spells of dizziness or shortage of breath?/ 11. Have you been treated during the past year for diabetes, heart/ trouble, kidney disease or tuberculosis?/ 12. Is there anything special about your physical condition that/ should be called to the doctor's attention?" printed on reverse.
- Missing
- none.
- Finish
- BLACK PRINT ON WHITE PAPER.
- Decoration
- N/A
CITE THIS OBJECT
If you choose to share our information about this collection object, please cite:
Unknown Manufacturer, Archival collection, between 1920–1948, Artifact no. 1981.0489, Ingenium – Canada’s Museums of Science and Innovation, http://collections.ingeniumcanada.org/en/item/1981.0489.002/
FEEDBACK
Submit a question or comment about this artifact.
More Like This
























1981.0489.002